
 Discussion
Discussion
Glioma overview
Last updated Dec. 18, 2024, by Lindsey Shapiro, PhD
 Fact-checked by Ana de Barros, PhD
Fact-checked by Ana de Barros, PhD
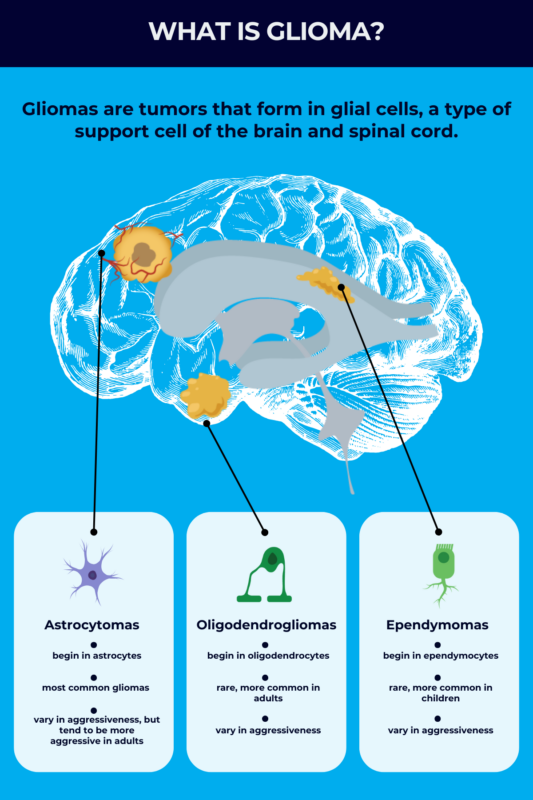
Gliomas are a group of brain tumors that arise from glial cells, a type of support cell of the central nervous system, or CNS, which comprises the brain and spinal cord.
They make up about one-quarter of all tumors that start in the brain (primary brain tumors), occurring in about 6.6 per 100,000 people every year. They also account for more than 80% of all malignant, or cancerous, brain tumors.
Gliomas vary widely in their aggressiveness, or grade, with some slow-growing and others highly aggressive. Treatment for malignant gliomas often relies on a combination of surgery and other approaches such as chemotherapy and radiation. The success of treatment and the resulting prognosis varies widely by glioma type and grade.
What is a glioma?
Gliomas are a group of tumors that start in glia, the cells that support and protect nerve cells in the CNS. They arise when random DNA mutations in glial cells cause their uncontrolled growth. Glioma tumors can form and grow anywhere in the CNS, but they most often occur in the cerebral hemispheres — the largest and outermost part of the brain.
Contrasting with most other tumors, gliomas won’t typically spread outside the CNS to the rest of the body, so they are not staged as other cancers are. Instead, these tumors are given a grade, depending on how abnormal the tumor cells appear compared with healthy brain cells, and how likely they are to grow and invade healthy brain tissue.
Malignant tumors can arise on their own, or can develop from benign, or noncancerous, tumors that acquire new cancer-driving genetic mutations. Cells from malignant gliomas, while resembling glia, are not able to perform the normal specialized functions that glia would.
Types
Traditionally, gliomas have been categorized into three main types based on the specific cells from which they arise:
- Astrocytomas begin in astrocytes, a class of star-shaped glia involved in many CNS processes.
- Oligodendrogliomas start in oligodendrocytes, the glial cells responsible for producing a protective substance called myelin that coats nerve cells.
- Ependymomas begin in ependymocytes, which line the fluid-filled cavities of the brain and spinal cord.
Astrocytomas
Astrocytomas are the most common type of glioma and can vary widely in aggressiveness. Glioblastomas, the most common type of primary brain tumor found in adults, are a very aggressive and fast-growing type of astrocytoma. Astrocytomas are also the most common type of brain tumor found in children, but they’re usually less aggressive in pediatric populations.
The most common astrocytoma in children is a benign form called pilocytic astrocytoma. However, there are rare and aggressive types, such as diffuse midline glioma — a subtype of diffuse intrinsic pontine glioma (DIPG) or pons glioma — that mainly affect pediatric populations.
Pleomorphic xanthoastrocytoma (PXA) and anaplastic astrocytoma are two other rare forms of astrocytoma with distinct characteristics. PXA predominantly affects young males, exhibits slow growth, and typically has favorable outcomes. Anaplastic astrocytoma, meanwhile, generally affects adults between the ages of 30 and 50, is aggressive, and may have a poorer prognosis.
Oligodendrogliomas
Oligodendrogliomas are a rare type of glioma, accounting for 5% to 15% of all gliomas and about 1% to 2% of all brain tumors. This type can be slow-growing or more aggressive. These tumors are more common in adults than children, and are considered to be among the more treatable types of brain cancer.
Ependymomas
Ependymomas are also quite rare, making up about 2% of all brain tumors. They’re more common in children than adults, and can vary in aggressiveness.
Other types
Some gliomas contain multiple cell types, usually astrocytes and oligodendrocytes, and are called mixed gliomas. There also is another very rare type of glioma that contains both glia and nerve cells. This is called a ganglioglioma and is usually benign, although some can become malignant and be very aggressive.
Because classifying gliomas is often more complex than simply determining what cell type they arise from, the World Health Organization developed a classification system for categorizing them and other brain tumors. This system relies on more detailed molecular and genetic profiling of the tumors. Doctors also can use these classifications to better tailor treatment approaches.
Grades
Doctors often classify how aggressive gliomas and other brain tumors are based on the microscopic structure of the tumor cells, as well as their molecular and genetic characteristics. This is done with a grading system that ranges from 1-4, with grades 1-2 corresponding to low grade, or less aggressive, tumors, and grades 3-4 corresponding to high grade, or more aggressive, ones.
- Grade 1 tumors usually contain normal-looking cells and grow slowly without invading nearby tissue. These tumors are considered benign.
- Grade 2 tumors look less like normal cells. While they still grow slowly, they have the potential to spread to nearby tissue and progress to a higher grade.
- Grade 3 tumors contain cells that look abnormal and can spread to other nearby parts of the CNS. They’re considered malignant. All oligodendrogliomas are considered Grade 2 or 3.
- Grade 4 tumors have highly abnormal cells and the tumor grows rapidly. These malignant tumors are likely to spread more widely and to return after treatment. These tumors form new blood vessels to support their rapid growth and have areas of dead cells, called necrosis, in their center. All glioblastomas are grade 4.
The grade of a tumor also can change over time. When a low-grade tumor becomes more aggressive, it is known as a malignant transformation. Most gliomas in children are considered low grade and don’t usually progress to become high grade. Most gliomas in adults are high grade, and low grade tumors in adults are more likely to have a malignant progression.
Causes and risk factors
In most cases, the exact reason why a glioma develops is not known, and research has not found anything specific that a person can do to prevent the disease.
The development of gliomas is associated with certain DNA mutations in the cancer cells, but these mutations generally happen randomly, or de novo, and aren’t inherited. It is very rare for gliomas to run in families, but in a small number of cases, they are linked to inherited genetic syndromes.
Some research suggests that prior exposure to certain toxins or ionizing radiation, a type of radiation with enough energy to affect atoms, could increase the risk of gliomas. Exposure to ionizing radiation can come from radiation therapy during cancer treatment, occupational exposures — such as working in a power plant or medical imaging facilities — or from natural sources such as soil, water, or vegetation.
Age also can influence the risk of glioma, as they most commonly occur in older adults, ages 65 and older, and in younger children, or those younger than age 12. These tumors are also slightly more likely to affect men than women, and are more common in white people.
Symptoms
Glioma symptoms are similar across disease types, but can vary depending on where the tumor is located. Symptoms often appear slowly and may be subtle at first. The development of more noticeable symptoms is often a consequence of the tumor growing and pressing on nearby brain tissue.
The most common symptoms of gliomas include:
- headaches
- seizures
- nausea and vomiting
- vision or hearing problems
- speech issues
- cognitive problems, including trouble with thinking, learning, or memory
- personality changes or irritability
- mobility or balance problems
- dizziness
- weakness and numbness on one side of the body, known as hemiparesis.
In some cases, low grade gliomas don’t cause any noticeable symptoms, but are caught on imaging scans conducted for other reasons.
Seizures are among the most common low grade glioma symptoms in adults and children. While seizures are often thought of as episodes of falling to the floor and shaking, they are often much more subtle — and even barely noticeable — with a low grade glioma. Signs of a seizure could include experiencing unusual smells, anxiety, feeling as though time was lost or having deja vu, difficulty speaking, confusion, numbness, or vision problems.
Another early warning sign of a low grade glioma may be a persistent headache, which can be dull and throbbing or sharp and stabbing.
High grade tumors, on the other hand, may cause more severe symptoms, including worsening headaches with nausea and vomiting — especially ones that are very intense in the mornings or that wake a person up at night. Such tumors also may cause seizures that are difficult to control, and progressively worsening neurological issues like loss of coordination, personality and behavior changes, and vision problems.
The specific symptoms a person experiences also will vary depending on where exactly the tumor resides.
- Tumors in the cerebellum, or the back part of the brain that controls coordination and balance, can cause trouble walking, problems with precise movement, swallowing issues, and changes in speech rhythm or eye movements.
- In the front part of the brain, which controls functions such as emotions, personality, and impulse control, tumors can affect thinking, personality, and language.
- Tumors near cranial nerves can lead to hearing loss, numbness, pain, or weakness in the face, as well as trouble swallowing.
- Tumors in the part of the brain that controls movement and sensation can lead to weakness or numbness, while tumors near language centers can cause issues with speech and language comprehension.
- Spinal cord tumors can cause numbness, weakness, coordination issues, or bladder and bowel problems.
As they grow, gliomas can ultimately cause serious and life-threatening complications, such as:
- bleeding in the brain, also called a hemorrhage
- brain herniation, in which brain tissue moves outside its normal position in the skull
- buildup of fluid in the brain
- increased pressure inside the skull
- seizures
- deep vein thrombosis, or the development of blood clots in deep veins, such as those in the legs, that can migrate to the lungs and block blood flow (pulmonary embolism).
Diagnosis
To reach a glioma diagnosis, doctors will first conduct a thorough medical history, along with a physical and neurological exam. A clinician will test a person’s vision, hearing, balance, strength, coordination, and reflexes.
If a patient shows signs suggestive of a glioma, the next step is to perform imaging scans, such as an MRI or CT scan, to look for any tumors. If a mass appears in imaging scans, doctors will finalize the diagnosis with a biopsy, in which a sample of the tumor tissue is collected and analyzed.
A biopsy involves cutting a small hole in the skull and inserting a small needle into the tumor to remove a sample. An analysis of the tissue will help determine if the glioma is cancerous, what type of cells it involves, and its grade. Such evaluations can also identify molecular and genetic features of the tumor that determine how it needs to be treated.
In situations in which a patient will undergo surgery to remove the brain tumor, it might not be necessary to perform a biopsy beforehand, as the tumor can be examined and diagnosed during the surgical procedure itself.
Detecting and treating gliomas in their early stages can increase survival rates and preserve cognitive function. Early intervention allows for less invasive treatment options, ultimately improving the patient’s overall quality of life.
Treatment
Glioma treatment will depend on the type of glioma, as well its size, location, and grade. Treatment also will be based on any health factors specific to the individual patient. Based on these factors, the person’s healthcare team will work together with the patient to come up with an optimal treatment plan.
In most cases, surgery to remove as much of the tumor as possible is the preferred first-line brain cancer treatment. Even when a tumor is benign, patients may still require surgery, especially if the tumor is pressing on healthy brain tissue and causing problems.
It can be hard to completely remove a glioma, especially when the tumor is difficult to reach without damaging healthy brain tissue, and/or when it’s located in very delicate areas. Such factors might mean that the tumor can only partially be removed, or surgery might not be possible at all.
Low grade tumors are often effectively treated with surgery. For high grade tumors, additional treatments will usually follow surgery, with the aim of destroying any remaining cancer cells. This follow-up treatment is called adjuvant therapy. Such treatments might also be used as the primary approach if surgery is not possible.
These treatment options may include:
- chemotherapy, a class of medications that stop the growth of cancer cells
- radiation therapy, in which beams of powerful energy are used to kill tumor cells
- tumor treating fields therapy, in which a portable device placed on the head delivers electrical energy through the skin to kill tumor cells
- targeted therapy, a class of medications that target specific changes in cancer cells that make them different from healthy cells.
In addition to primary cancer treatments, patients may receive a variety of supportive care measures, also known as palliative care. These measures aim to help ease symptoms, prevent complications, and reduce radiation or chemotherapy side effects. They may include:
- medications to control seizures
- steroids to ease brain swelling
- medicines to help with cognitive issues
- anti-nausea treatments
- pain management
- physical, speech, or occupational therapy to help regain skills lost from brain cancer or treatment.
There may be ongoing clinical studies that are testing new treatment approaches for gliomas. If interested, patients should talk with their doctors about whether there are any studies for which they are eligible to participate.
Life expectancy and survival rate
Glioma survival rates vary substantially based on the cancer type and grade, as well as general health factors. Overall, low grade tumors for which complete surgical removal of the cancer is possible are associated with the best survival rates, with many patients being cured. However, a high grade glioma brain tumor is associated with substantially lower survival rates.
Treatment for people with a grade 1 glioma is usually successful, especially when the tumor can be completely removed with surgery. The 5-year survival rate — the percentage of people still alive five years after their diagnosis — is about 95%. That rate drops to approximately 40%-50% for grade 2 gliomas, and 25%-30% for grade 3 gliomas.
Survival for glioma grade 4, such as glioblastoma, is the lowest of all glioma types, with about 5%-10% of patients surviving five years or more past their diagnosis.
Often, glioblastoma is resistant to treatment, and disease management is usually focused on palliative care to ease symptoms and improve comfort. Patients with a glioblastoma live, on average, about 12-18 months from their diagnosis.
Still, every person’s clinical situation is unique, and age and overall health status will influence an individual’s brain cancer life expectancy. The older a person is at the time of diagnosis and treatment, the worse that individual’s outlook tends to be.
Support and resources
Dealing with a glioma diagnosis and managing the changes to daily life that come with it can be overwhelming, but there are a few things a person can do to make living with brain cancer easier. Becoming educated about the disease and its treatment options — and staying in routine communication with one’s healthcare team — can help a patient feel more in control over the situation.
Brain cancer and its treatment can also damage healthy brain tissue. Physical, speech, or occupational therapy may be key for managing these neurological changes and making daily life with glioma easier. Professionals in these fields can work with patients to design personalized lifestyle changes that may help in their particular case.
Staying on top of one’s mental health — especially if faced with a terminal cancer diagnosis — is also critical for living as well as possible with a glioma. It’s important for patients to build a reliable support network of people who can help them deal with both the physical and emotional changes that will arise due to glioma. Some sources of support may include:
- family and friends
- mental health professionals, including therapists or counselors
- glioma support groups.
There are various glioma support organizations that offer online and in-person resources for those managing a glioma diagnosis. These include the:
- National Brain Tumor Society
- Glioblastoma Foundation
- Brain Tumor Network
- American Brain Tumor Association.
Patients can ask their doctors or social workers for a list of support resources in their area of residence. Rare Cancer News also aims to serve as a trusted resource for those living with glioma, offering the most up-to-date news and educational materials about the condition.
Rare Cancer News is strictly a news and information website about the disease. It does not provide medical advice, diagnosis, or treatment. This content is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this website.

Related articles
-
Discussion
-
 Discussion
Discussion
-
 Discussion
Discussion
-
 Discussion
Discussion
-
 Discussion
Discussion
-
Discussion